Looking for Expert-Level VA Claim Answers?📱Call Us Now! 737-295-2226
If you’re eligible and you build your VA claim with the right evidence, it’s provable. The VA’s service-connection standard is “at least as likely as not” (50/50)—and ties go to the veteran. No evidence = denial or underrating.
In this expert-level guide from Brian Reese, he’ll teach you exactly what helps win: a current diagnosis, in-service event/injury/disease, a medical nexus connecting the two, and documented severity mapped to the rating criteria.
You’ll also learn the smartest paths to service connection (direct, secondary, presumptive, aggravation, §1151), field-tested pro tips to avoid common pitfalls, and how to bounce back from denials using the right appeal lane with new and relevant evidence.
Let’s get started!
Table of Contents
Summary of Key Points
- Every VA claim is provable—if you’re eligible and build the right evidence. The VA’s standard is “at least as likely as not” (50/50), so ties go to the veteran; no evidence = denial or underrating.
- Review the VA Claims Insider Golden Circle. Assemble all four: current diagnosis, in-service event/injury/disease (or aggravation), a medical nexus linking the two, and documented severity mapped to the rating criteria.
- Choose the correct VA service connection path. Use the best legal theory for your facts—Direct, Secondary, Presumptive, Aggravation, or §1151—and avoid common pitfalls with clean claim sequencing, tight organization, and evidence that speaks the VA’s language.
- If denied, re-attack with the right appeal lane. File an Increase when symptoms worsen, or pursue Supplemental (new & relevant evidence), HLR, or Board—closing the exact gap (often nexus, current diagnosis, or severity).
Part I — Eligibility: The First Gate You Must Clear First
Before the VA even looks at your medical evidence, you must be eligible for VA disability benefits.
- Character of service: Generally Honorable (certain OTH/General cases can still qualify—complex but possible).
- Qualifying service: Active duty (some Guard/Reserve periods count if you were on federal active orders).
If you’re not eligible under the law, the rest doesn’t matter. Confirm this first by looking at your DD 214.
Part II — The VA Claims Insider Golden Circle (4 Must-Prove Elements with Examples)
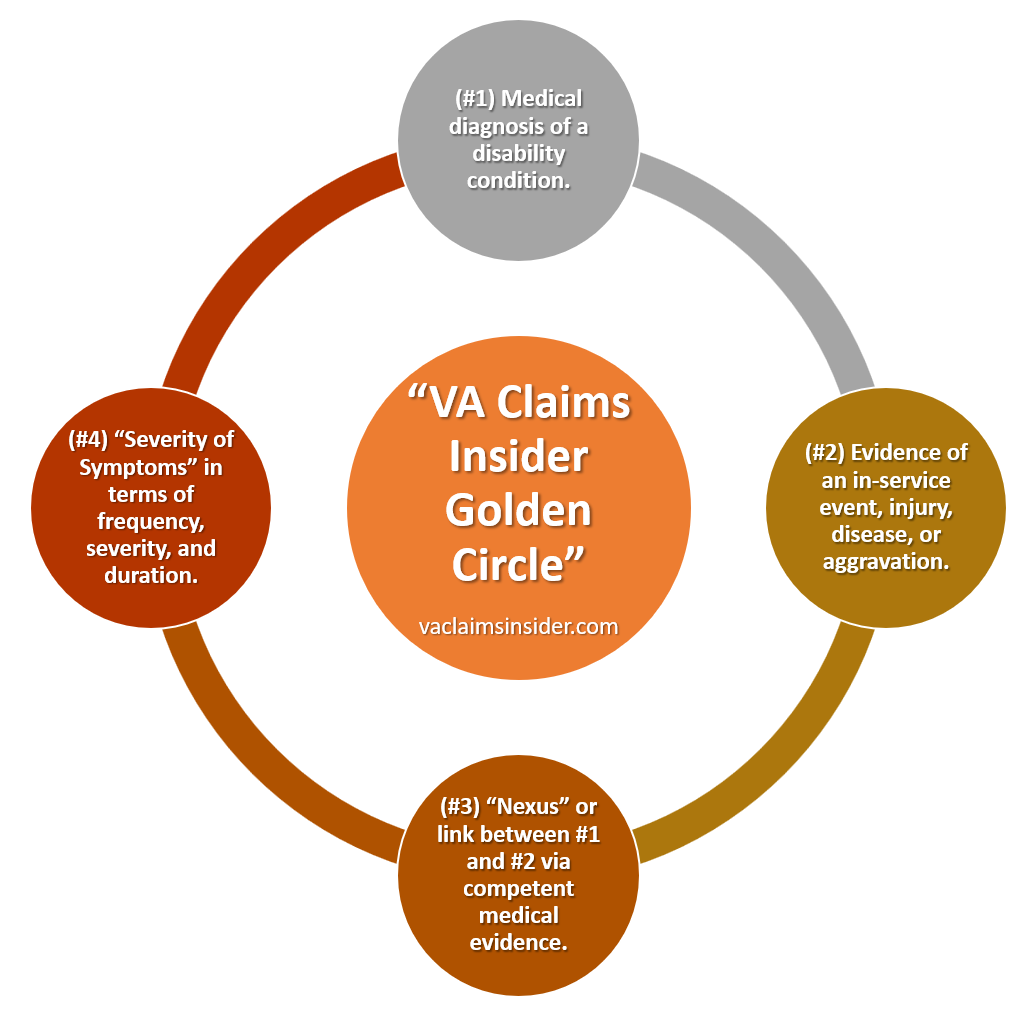
Think of the VA Claims Insider Golden Circle as a decision tree. If the answer is “yes,” move to the next element:
1. Current Diagnosis (documented in a medical record)
You need a medically recognized current diagnosis in VA or private records (ideally within the last 12 months).
- Examples:
- Tinnitus confirmed on audiology note.
- Lumbar strain on orthopedic exam with ICD-10 code.
- PTSD diagnosed by a qualified mental health clinician using DSM-5 criteria.
- Obstructive sleep apnea confirmed by a polysomnography (sleep study).
- Pro Tip: If your last diagnosis is old, consider getting an updated one to lock in “current.”
2. In-Service Event, Injury, Disease (or Aggravation)
Show something happened in service—or a pre-existing condition worsened beyond natural progression.
- Examples:
- Noise exposure from aircraft flight line (documented MOS with high noise probability).
- Knee injury during PT; line-of-duty note or STR entry.
- Burn-pit exposure during a deployment (location and dates).
- Aggravation: Pre-service asthma worsened during Iraq deployment (increased meds, ER visits).
- MST markers: sudden performance drop, duty transfer, counseling/chaplain notes when no formal report exists.
- Pro Tip: When STRs are thin, use buddy letters, unit records, award narratives, or deployment orders to corroborate.
3. Nexus (the medical link or connection between #1 and #2)
A clinician explains why your current diagnosis is “at least as likely as not” related to the in-service event/aggravation. This is the bridge that wins or loses most claims.
- Examples:
- Tinnitus ↔ Flight-line noise: “Veteran’s current tinnitus is at least as likely as not due to high-decibel aircraft exposure in service.”
- Migraines ↔ PTSD: “Headaches began after trauma in service; medical literature supports PTSD-associated migraines—at least as likely as not.” (Secondary connection)
- Radiculopathy ↔ Lumbar strain: “Current left-leg radiculopathy is secondary to service-connected lumbar spine condition.” (Secondary/aggravation)
- Sleep apnea ↔ Rhinitis/Deviated septum: “Upper-airway obstruction from service-connected rhinitis aggravates OSA—at least as likely as not.” (Secondary/aggravation)
- Presumptive: Vietnam boots-on-ground + Type 2 diabetes: nexus is presumed once service/exposure criteria and diagnosis are met.
- Pro Tip: Ask for a reasoned nexus (DBQ or letter) that cites facts (onset, continuity), mechanisms, and—when useful—supporting literature. Bare conclusions are weak.
4. Severity (Frequency • Severity • Duration) → Your VA Rating Percentage
Once service connection is established, your VA rating percentage depends on how often symptoms occur, how bad they are, how long they last, and functional impact (work, life, social functioning).
- Examples:
- Knee condition: Limited flexion, instability on testing, frequent flare-ups documented by ortho; impacts stair climbing at work.
- PTSD: Panic attacks more than once a week, impaired work relationships, sleep disturbance; therapy notes and employer statements.
- GERD: Persistent reflux, regurgitation, substernal pain; requires continuous meds; impacts sleep and diet.
- TBI residuals: Cognitive deficits on neuropsych testing; headaches 3–4×/week; memory issues affecting job performance.
- Pro Tip: Keep a symptom diary. Translate daily impact into the Rating Schedule’s language (e.g., “more than once weekly,” “requires continuous medication,” “marked interference with employment”). Include spouse/caregiver statements when they observe flares or limitations.
Elements #1–#3 are the classic Caluza Triangle elements (diagnosis, in-service event, nexus). Element #4 determines your final VA rating percentage once service connection is granted.
Part III — The 5 Legal Paths to Service Connection
You don’t have to force every claim down a single road. Pick the right legal theory of service connection:
- Direct: Began in service (e.g., knee injury on deployment).
- Secondary: Proximately due to, caused, or aggravated by a service-connected condition (e.g., back → radiculopathy; PTSD → migraines; tinnitus → headaches).
- Presumptive: VA presumes a link based on exposure/time/locations (e.g., Agent Orange, Gulf War, Burn Pits, Camp Lejeune, certain chronic diseases within one year).
- Aggravation: Pre-service condition permanently worsened beyond natural progression due to service.
- 38 U.S.C. § 1151: Additional disability from qualifying VA treatment—paid as if service-connected. This is rare.
Part IV — Easy VA Claims to Get Approved
Some VA claims are easier than others to get approved. With 1,000+ ratable VA disabilities, the VA system can feel overwhelming. You might not even know what you’re eligible for.
The good news: these top 25 easiest VA claims are generally easier to prove when you know the evidence the VA weighs most—diagnosis, in-service event, nexus, and severity of symptoms.
List of the 25 Easiest VA Disability Claims
- Tinnitus
- Mental Health Conditions
- Presumptive Conditions
- Musculoskeletal Conditions
- Migraines (Headaches)
- Erectile Dysfunction (ED) & Female Sexual Arousal Disorder (FSAD)
- Irritable Bowel Syndrome (IBS)
- Radiculopathy
- Plantar Fasciitis
- Flat Feet (Pes Planus)
- Paralysis of the Sciatic Nerve (Sciatica)
- Scars, General
- Degenerative Arthritis of the Spine
- Asthma
- Diabetes Type 2
- Cancer
- Arthritis
- Gastroesophageal Reflux Disease (GERD)
- Hypertension (High Blood Pressure)
- Degenerative Disc Disease (DDD)
- Carpal Tunnel Syndrome (CTS)
- Chronic Fatigue Syndrome (CFS)
- Fibromyalgia
- Hemorrhoids
- Sleep Apnea
Part V — The 6 Critical Factors That Decide Approval of Your VA Claim
- Honorable discharge (eligibility).
- Qualifying active service (eligibility).
- Current diagnosis (in a medical record).
- In-service event/injury/disease (or aggravation).
- Nexus opinion using “at least as likely as not.” Tie goes to the veteran. When evidence is in approximate balance (50/50), the law says grant.
- Severity documented to the VA rating schedule (frequency, severity, duration, and functional impact on work/life/social functioning).
Part VI — Evidence That Moves the Needle (Use This Checklist)
Medical:
- Current diagnosis (ICD-10) from VA or private clinician
- Treatment notes showing onset, continuity, flares, and functional loss
- Nexus letter/DBQ that addresses why it’s at least as likely as not (medical reasoning, literature, exposures)
Service/Exposure:
- STRs, line-of-duty reports, incident logs
- Duty MOS noise exposure tables, deployment/exposure records
- Buddy statements (identify, describe, and date the event/observations)
Severity/Impact:
- Symptom diary (frequency • severity • duration)
- Work/life/social functioning limitations, accommodations, missed time
- Caregiver notes, spouse/partner observations
- Objective testing where applicable (audiology, MRI, PFTs, sleep study, labs)
For MST/Unreported Events:
- “Markers” (buddy letters, personal statement, sudden performance decline, UCMJ events, transfer requests, counseling, chaplain notes, medical visits, pregnancy/STD tests, substance changes)
Part VII — VA Claim Sequencing (Don’t Create Your Own Headwinds)
- Secondary claims: It’s a best practice to service-connect the primary first (even at 0%), then file the secondary. This avoids chain denials and clarifies the nexus. Make it easy for the VA rater to approve your secondary claim.
- Combined conditions: Disaggregate diagnoses where the rating schedule treats them differently (e.g., orthopedic + radiculopathy + scars).
- Increases: When symptoms worsen, file for an increase with new and relevant evidence tied to the VA rating criteria in 38 CFR Part 4 the Schedule for Rating Disabilities.
Part VIII — Common Pitfalls (and Easy Fixes)
- No current diagnosis: Get evaluated—symptoms alone rarely win. A current diagnosis within the past 12 months is helpful.
- Assuming the VA will infer nexus: It won’t. Obtain a competent, evidence-based nexus letter.
- Thin in-service proof: Bolster with buddy letters and circumstantial documentation. You can also write a strong personal statement to support your claim.
- Under-documenting severity: Track flares, work limits, and life/relationship impact—speak the rating schedule’s language.
- Submitting a document dump: Organize and label. Make it easy for the rater to say “yes.” Less is more. More is not more!
Part IX — Who Is Not Eligible? (High-Level Overview)
Certain legal bars generally prevent compensation (consult a VSO/attorney for nuances):
- Dishonorable discharge (or certain statutory bars under 38 C.F.R. § 3.12)
- Disabilities due to a veteran’s own willful misconduct
- Desertion, mutiny, spying/treason, or AWOL ≥180 days without compelling circumstances
- Conscientious objector who refused duty after induction (specific circumstances)
There are exceptions and fact-specific analyses. Don’t self-disqualify—get a professional review.
Frequently Asked Questions (FAQs)
Are there VA claims that cannot be proven?
There are no “unprovable” VA claims. If you’re eligible and you build the right evidence, your claim is provable. The VA’s legal standard is “at least as likely as not” (50/50), which means a tie goes to the veteran. Winning comes down to assembling four pieces: current diagnosis, an in-service event or aggravation, a medical nexus linking the two, and documented severity that maps to the rating criteria. No evidence—or the wrong evidence—leads to denial or underrating.
Who is eligible for VA disability benefits?
Eligibility generally requires an Honorable (or qualifying) character of discharge and qualifying active duty service; some Guard/Reserve periods count if you were on federal active orders. If eligibility is unclear (e.g., General/OTH, extended AWOL, misconduct issues), get a professional review before filing—don’t self-disqualify.
What is the VA’s burden of proof?
The VA uses the “at least as likely as not” standard. You don’t need to prove your case beyond a reasonable doubt; you need competent evidence showing a 50/50 connection between your condition and service. When the evidence is in approximate balance, the benefit of the doubt doctrine says the VA should grant.
What is the VA Claims Insider “Golden Circle”?
It’s a simple win framework: (1) current diagnosis, (2) in-service event/injury/disease or aggravation, (3) a medical nexus opinion linking 1 and 2 at 50/50, and (4) severity documented to the rating schedule (frequency, severity, duration, and functional impact). Steps 1–3 get you service-connected; step 4 determines your percentage.
Which VA claims are typically easier to win?
Claims with clear documentation and continuity tend to move faster: tinnitus/hearing loss with documented noise exposure and audiology, scars or straightforward musculoskeletal injuries with line-of-duty notes, and presumptives where you meet service/exposure criteria (e.g., Agent Orange, Gulf War, toxic exposures). “Easier” still requires a current diagnosis and the right records.
Which VA claims are often harder—and why?
Hearing loss is one of the most difficult claims to get service connected and rated above 0%. PTSD VA claims can also be challenging without a documented stressor or markers; GWI/CFS/fibromyalgia and other diffuse or delayed-onset conditions need meticulous symptom tracking and a strong medical rationale for latency and continuity. Harder does not mean impossible—it means your nexus and evidence must be more robust, organized, and specific.
Do presumptive conditions still require evidence?
Yes. Presumptives lower the nexus burden (you aren’t required to prove a nexus), but you still need a current diagnosis and proof that you meet the service/exposure window (location, dates, unit). For example, a Vietnam “boots on ground” veteran with Type 2 diabetes still needs the diagnosis and qualifying service to trigger the presumption.
What is a nexus letter—and do I need one?
A nexus letter from a private provider (and/or a DBQ medical opinion from a C&P examiner) is a clinician’s medical explanation that your condition is at least as likely as not related to service or to a service-connected condition. Strong opinions cite facts (onset, mechanism, continuity), reference medical literature when helpful, and explain aggravation where relevant. Bare conclusions (“it’s related”) are weak.
Can lay statements and buddy letters help me win?
Absolutely. When service records are thin, credible lay evidence for your VA claim can corroborate events, exposures, and observable symptom patterns. Effective statements are specific (who/what/when/where), avoid medical conclusions, and align with medical records. Pairing lay statements with clinical notes materially strengthens your file.
What if my symptoms worsen or I was denied before?
If symptoms worsen, file for an increase with fresh evidence mapped to the rating criteria (frequency, severity, duration, and functional loss). If denied, choose the right appeal lane—Supplemental (with new and relevant evidence), Higher-Level Review, or Board—and fix the actual gap that caused the denial (often missing diagnosis, weak nexus, or poor severity documentation). View the difference between HLR and Supplemental Claim.
Conclusion & Wrap-Up
There are no “unprovable” VA claims—only claims missing the right evidence or the right legal theory. If you’re eligible and you build your claims file around the VA Claims Insider Golden Circle (Diagnosis → In-Service Event/Aggravation → Nexus → Severity), you’ve given the rater everything needed to say yes. At 50/50, the law breaks the tie in your favor.
Final takeaways:
- Eligibility first. Confirm character of service and qualifying active duty before you do anything else.
- Win the elements. Lock in a current diagnosis, prove the in-service event/aggravation, secure a reasoned nexus (“at least as likely as not”), and document severity in the VA’s language (frequency, severity, duration, functional loss).
- Choose the right path. Direct, Secondary, Presumptive, Aggravation, or §1151—don’t force the wrong theory.
- Evidence > volume. Organized, relevant, and labeled beats a document dump every time.
- Denied ≠ done. Re-attack with the correct appeal lane and new & relevant evidence that fixes the exact gap.
Want Expert-Level VA Claim Help? WE GOT YOUR SIX!
- VA Claims Insider is the #1 most trusted name in VA disability claims.
- Work directly with a VA Claims Insider Coach who can help lead you to VA claim victory.
- 25,000+ disabled veterans served in our membership programs since 2016.
- 30% average rating increase for veterans who complete our #1 rated Elite program.
- 4.6/5.0 average rating out of 6,500+ total reviews; over 5,500 5-star reviews.
About the Author

Brian Reese
Brian Reese is a world-renowned VA disability benefits expert and the #1 bestselling author of VA Claim Secrets and You Deserve It. Motivated by his own frustration with the VA claim process, Brian founded VA Claims Insider to help disabled veterans secure their VA disability compensation faster, regardless of their past struggles with the VA. Since 2013, he has positively impacted the lives of over 10 million military, veterans, and their families.
A former active-duty Air Force officer, Brian has extensive experience leading diverse teams in challenging international environments, including a combat tour in Afghanistan in 2011 supporting Operation ENDURING FREEDOM.
Brian is a Distinguished Graduate of Management from the United States Air Force Academy and earned his MBA from Oklahoma State University’s Spears School of Business, where he was a National Honor Scholar, ranking in the top 1% of his class.