Looking for Expert-Level VA Claim Answers?📱Call Us Now! 737-295-2226
In this Ultimate Guide, we’ll explore how to get a VA Rating for PTSD even if you’ve already filed or been denied PTSD benefits in the past.
Your final VA Disability Rating for PTSD depends upon the Frequency, Severity, and Duration of symptoms to include “HOW” those symptoms impact your “Occupational and Social Impairment.”
VA Disability for PTSD has ratings that range from 0 percent to 100 percent with breaks at 10 percent, 30 percent, 50 percent, and 70 percent.
PTSD is the only ratable mental health condition that requires a “Stressor Event” by the VA (more on that below).
Also note that it’s highly unlikely to receive a separate rating for PTSD if you’re already rated for another mental health condition due to the avoidance of pyramiding, and the overlap of symptoms across multiple diagnoses.
We’ve broken down this post into 7 Chapters to help guide you on your PTSD VA claim journey.
Okay, let’s jump into this expert-level guide for getting service connected disability benefits for PTSD.
- Chapter 1: VA Claims for PTSD Introduction
- Chapter 2: The Importance of PTSD Stressors
- Chapter 3: Service Connection for PTSD
- Chapter 4: VA Disability Ratings for PTSD
- PTSD Basic Eligibility Criteria
- How Do I Get a VA Disability Rating for PTSD?
- How Do I Increase VA Disability PTSD?
- What is the Reasonable Doubt Rule for PTSD?
- How Does the VA Rate PTSD?
- What is the PTSD Compensation Chart?
- What is the PTSD Rating Scale?
- 0 Percent Rating for PTSD
- 10 Percent VA Rating for PTSD
- 30 Percent VA Disability Rating for PTSD
- 50 Percent PTSD VA Rating
- 70 Percent VA Rating for PTSD
- 100 Percent VA Disability Rating for PTSD
- What Are the Two Important Rules Affecting PTSD VA Ratings?
- What Should I Expect at a C&P Exam for PTSD?
- What Questions Will I Get Asked At a PTSD C&P Exam?
- WATCH: What You Need to Know For Your PTSD C&P Exam
- Chapter 5: The 31 Symptoms of a PTSD VA Disability Rating
- What Are the PTSD Symptoms Reviewed by the C&P Examiner?
- #1. Depressed mood
- #2. Anxiety
- #3. Suspiciousness
- #4. Panic attacks that occur weekly or less often
- #5. Panic attacks more than once a week
- #6. Near-continuous panic or depression affecting the ability to function independently, appropriately, and effectively
- #7. Chronic sleep impairment
- #8. Mild memory loss, such as forgetting names, directions, or recent events
- #9. Impairment of short- and long-term memory, for example, retention of only highly learned material, while forgetting to complete tasks
- #10. Memory loss for names of close relatives, own occupation, or own name:
- #11. Flattened affect
- #12. Circumstantial, circumlocutory, or stereotyped speech
- #13. Speech intermittently illogical, obscure, or irrelevant
- #14. Difficulty in understanding complex commands
- #15. Impaired judgment
- #16. Impaired abstract thinking
- #17. Gross impairment in thought processes or communication
- #18. Disturbances of motivation and mood
- #19. Difficulty in establishing and maintaining effective work and social relationships
- #20. Difficulty adapting to stressful circumstances, including work or a work like setting
- #21. Inability to establish and maintain effective relationships
- #22. Suicidal ideation
- #23. Obsessional rituals which interfere with routine activities
- #24. Impaired impulse control, such as unprovoked irritability with periods of violence
- #25. Spatial disorientation
- #26. Persistent delusions or hallucinations
- #27. Grossly inappropriate behavior
- #28. Persistent danger of hurting self or others
- #29. Neglect of personal appearance and hygiene
- #30. Intermittent inability to perform activities of daily living, including maintenance of minimal personal hygiene
- #31. Disorientation to time or place
- Chapter 6: VA Disability Ratings for PTSD in 2024 – Frequently Asked Questions (FAQs)
- Can I get VA disability compensation for PTSD?
- Is PTSD a VA disability condition?
- What are the VA disability ratings for PTSD?
- Can I receive Special Monthly Compensation for PTSD?
- Can PTSD be Permanent and Total (P&T)?
- Can the VA reduce my VA disability rating for PTSD?
- How do I get a 100% VA disability for PTSD?
- Can I work with a 100% VA Rating for PTSD?
- Will PTSD affect my security clearance?
- Can I own a gun with a VA rating for PTSD?
- Chapter 7: Helpful VA Resources for PTSD
- About the Author
Chapter 1: VA Claims for PTSD Introduction
What is PTSD in Veterans?

Post-Traumatic Stress Disorder, or PTSD, is a mental health condition that some veterans develop after experiencing or witnessing a life-threatening event, such as a combat situation, a natural disaster, a car accident, or a sexual assault.
During the traumatic event, you may not have any control over what’s happening, and you may feel very afraid, in fact, you might have feared for your life.
Veterans who have gone through a traumatic event can develop PTSD.
Note that it’s completely normal to have upsetting memories, feel on edge, or have trouble sleeping after the traumatic event.
Initially, it may be hard to do daily activities you are used to doing, such as, go to work, go to school, or spend time with family and friends.
Most veterans start to feel better after a few weeks or months.
But for some veterans, PTSD symptoms may start later, or they may come and go over time.
If it’s been longer than a few months and thoughts and feelings from the trauma are upsetting you or causing problems in your life, you may have PTSD.
How Common is PTSD in Veterans?

It is estimated that U.S. military veterans are nearly four times as likely to develop PTSD as someone who didn’t wear the uniform.
According to the VA’s published statistics, the number of veterans with PTSD varies by service era:
- Operations Iraqi Freedom (OIF) and Enduring Freedom (OEF): About 11-20 out of every 100 Veterans (or between 11-20%) who served in OIF or OEF have PTSD each year.
- Gulf War (Desert Storm): About 12 out of every 100 Gulf War Veterans (or 12%) have PTSD each year.
- Vietnam War: About 15 out of every 100 Vietnam Veterans (or 15%) were currently diagnosed with PTSD at the time of the most recent study in the late 1980s, the National Vietnam Veterans Readjustment Study (NVVRS). It is estimated that about 30 out of every 100 (or 30%) of Vietnam Veterans have had PTSD in their lifetime.
Another cause of PTSD in the military can be Military Sexual Trauma (MST).
This is any sexual harassment or sexual assault that occurs while you are in the military.
MST can happen to both men and women and can occur during peacetime, training, or war.
Among Veterans who use VA healthcare:
- 23 out of 100 women (or 23%) reported sexual assault when in the military.
- 55 out of 100 women (or 55%) and 38 out of 100 men (or 38%) have experienced sexual harassment when in the military.
Note that there are many more male Veterans than there are female Veterans.
So, even though military sexual trauma is more common in women Veterans, over half of all Veterans with military sexual trauma are men.
What Are the Risk Factors For PTSD?

Any veteran can develop PTSD.
Some factors can increase the chance that a veteran will have PTSD, many of which are not under your control.
For example, having a very intense or long-lasting traumatic event (e.g., rocket attacks) or getting injured during the event can make it more likely that a veteran will develop PTSD.
PTSD is also more common after certain types of traumas, such as combat or sexual assault.
Personal factors, such as previous traumatic exposure, age, and gender can affect whether a veteran will develop PTSD.
What Are Common Signs and Symptoms of PTSD?
PTSD symptoms usually start soon after the traumatic event, but they may not appear until months or years later.
Your symptoms can also can ebb-and-flow over many years.
If the symptoms last longer than four weeks, cause you great distress, or interfere with your work or home life, you might have PTSD.
Generally, there are 4 types of PTSD symptoms, but they may not be the same for veteran.
Each veteran experiences symptoms of PTSD in their own way.
#1. Reliving the event (also called re-experiencing symptoms)
Memories of the traumatic event can come back at any time, and they can feel very real and scary.
- You may have nightmares.
- You may feel like you are going through the event again. This is called a flashback.
- You may see, hear, or smell something that causes you to relive the event. This is called a trigger. News reports, seeing an accident, or hearing fireworks are examples of triggers.
#2. Avoiding things that remind you of the event
You may try to avoid situations or veterans remind you of the trauma event.
You may even avoid talking or thinking about the event.
- You may avoid crowds because they feel dangerous.
- You may avoid driving if you were in a car accident or if your military convoy was bombed.
- If you were in an earthquake, you may avoid watching movies about earthquakes.
- You may keep very busy or avoid getting help so you don’t have to think or talk about the event.
#3. Having more negative thoughts and feelings than before the event
The way you think about yourself, and others may become more negative because of the trauma.
- You may feel numb—unable to have positive or loving feelings toward other veterans—and lost interest in things you used to enjoy.
- You may forget about parts of the traumatic event or not be able to talk about them.
- You may think the world is completely dangerous, and no one can be trusted.
- You may feel guilt or shame about the event, wishing you had done more to keep it from happening.
#4. Feeling on edge or keyed up (hyperarousal)
You may be jittery, or always alert and on the lookout for danger.
You might suddenly become angry or irritable.
- You may have a hard time sleeping.
- You may find it hard to concentrate.
- You may be startled by a loud noise or surprise.
- You might act in unhealthy ways, like smoking, abusing drugs or alcohol, or driving aggressively.
Chapter 2: The Importance of PTSD Stressors
What is a PTSD Stressor Event?

The primary difference between PTSD claims and other claims for mental health conditions is that PTSD always has a stressor.
Pro Tip: If you’re wondering if your PTSD stressor is strong enough, here’s a quick litmus test:
Did you fear for your life?
If yes, your stressor is strong enough to get a PTSD VA rating.
The VA must perform necessary claim development for PTSD and verify the claimant’s stressor event.
A PTSD stressor is a traumatic event (or series of events) in which an individual has been personally or indirectly exposed to actual or threatened:
- Death
- Serious injury, or
- Sexual violence
Claims can also be based on a stressor related to:
- An in-service PTSD diagnosis
- Personal assault
- Combat or former prisoner of war (FPOW) service
- Fear
- A stressful event unrelated to hostile military or terrorist activity
What Are the Different Types of PTSD Stressors?

PTSD stressor events generally fall into two categories:
#1. PTSD combat stressors AND
#2. PTSD non-combat stressors, which includes claims for Military Sexual Trauma (MST) related to assault or harassment.
Examples of PTSD Combat Stressors Include:
#1. Engaging in combat with the enemy

This category of stressor is reserved for veterans who participated in events constituting an actual fight or encounter with a military foe or hostile unit or instrumentality.
It includes presence during such events either as a:
- Combatant, or
- Service member performing duty in support of combatants, such as providing medical care to the wounded.
#2. Fear of hostile military or terrorist activity

This category of stressor includes experiencing or witnessing a combat-related event, the fear of an attack, or any terrorist-related activity.
- The veteran experienced, witnessed, or was confronted with an event or circumstance that involved
- actual or threatened death or serious injury, or
- a threat to the physical integrity of the Veteran or others, and
- The veteran’s response to the event or circumstances involved a psychological or psycho-physiological state of fear, helplessness, or horror
Examples of exposure to hostile military or terrorist activity include presence at events including:
- Actual or potential improvised explosive devices (IEDs)
- Vehicle-embedded explosive devices
- Incoming artillery, rocket, or mortar fire
- Small arms fire, including suspected sniper fire, or
- Attacks upon friendly aircraft
Pro Tip: Fear-based stressor criteria for PTSD was added at 38 CFR 3.304(f)(3) effective July 13, 2010, along with relaxed evidentiary standards for verifying PTSD stressors in accordance with VA Training Letter 10-05 (Revised).
References:
- Fear of hostile military and terrorist activity, see
- The liberalizing effect of 38 CFR 3.304(f)(3), see
- Ortiz v. McDonough, 6 F.4th 1267 (Fed. Cir. 2021), and
- M21-1, Part VIII, Subpart iv, 1.D.2.d.
What are the Special Requirements for PTSD Stressors Based on Areas of Potential Hostile Military or Terrorist Activity?
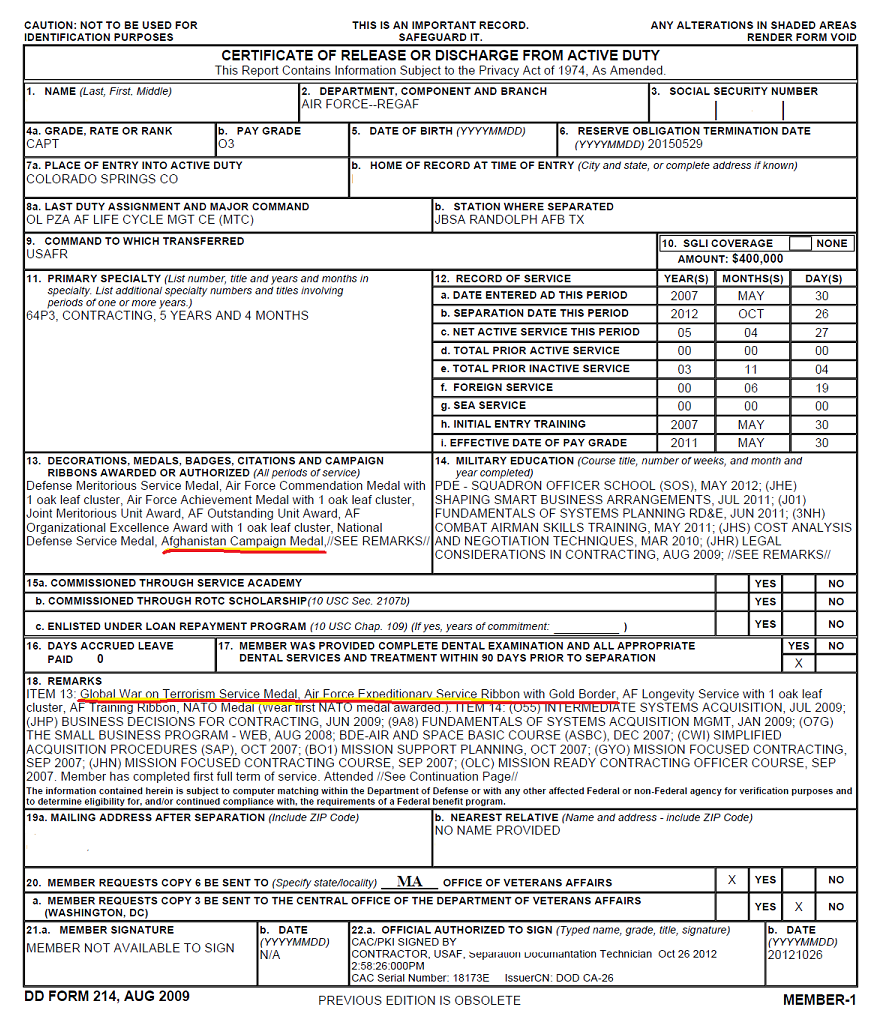
- Concede a stressor when the Veteran’s DD Form 214 or other service records show service in an area of potential hostile military or terrorist activity.
- Service personnel records must be requested prior to or concurrently with any necessary examination being ordered to avoid unnecessary delays in claims processing.
- The receipt of military awards such as, but not limited to, the Vietnam Service or Campaign Medal, Kuwait Liberation Medal, Iraq Campaign Medal, and Afghanistan Campaign Medal is generally considered evidence of service in an area of potential hostile military or terrorist activity.
- The receipt of military awards such as the National Defense Service Medal, Armed Forces Service Medal, and Global War on Terrorism (GWOT) Service Medal generally does not indicate service in locations that involve exposure to hostile military or terrorist activity because these are general medals that do not denote service in a particular area or campaign. If the Veteran served in an area of potential hostile military or terrorist activity, he/she/they likely would have received a more specific medal for such service.
- The GWOT Expeditionary Medal also does not necessarily indicate service in an area that would involve exposure to hostile military or terrorist activity. Consider that award and the other evidence of record to determine if there was service in an area of potential hostile military or terrorist activity before scheduling an examination.
- The fear-based stressor criteria are not met based on:
- Anticipation of future deployment to a location of hostile military or terrorist activity, or
- Learning of the death of another person when such death occurred remote from the Veteran in a location of hostile military or terrorist activity.
References:
- Establishing a stressor related to the fear of hostile military or terrorist activity, see M21-1, Part VIII, Subpart iv, 1.D.2.d
- When to proceed with an examination in a PTSD claim, see M21-1, Part VIII, Subpart iv, 1.C
- Requesting service personnel records from NPRC in PTSD claims, see M21-1, Part VIII, Subpart iv, 1.A.2.e, and
- Obtaining service records, see M21-1, Part III, Subpart ii, 2.
Examples of PTSD Non-Combat Stressors Include:

Non-combat stressor events involve specific incidents other than engaging in combat with the enemy or fear of hostile military or terrorist activity, including but not limited to:
- Natural disasters
- Life threatening disease of self or significant other
- Duty on burn ward
- Graves registration
- Witnessing the death, injury, or threat to the physical integrity of another person not caused by the enemy
- Actual or threatened death or serious injury, or other threat to one’s physical integrity not caused by the enemy
- Ship sinking, explosion, and/or plane crash during routine drills
- Friendly fire that occurs on a gunnery range during a training mission
- Personal assault including battery, rape, and sexual harassment
Pro Tips:
- The main distinction between a combat and non-combat stressor is that the non-combat stressor must always be corroborated with credible supporting evidence. The veteran’s lay statement, in the absence of any other credible evidence, cannot serve as evidence for verification of the stressor.
- Although a personal trauma stressor is generally related to a non-combat event, there are special criteria and considerations for personal trauma PTSD claims, which are provided in M21-1, Part VIII, Subpart iv, 1.B.
Concede a non-combat stressor event when credible supporting evidence:
- Documents the veteran’s participation in the event
- Indicates the veteran served in the immediate area and at the time in which the stressful event is alleged to have occurred, and
- Supports the description of the event
What Are the Special Requirements for PTSD MST Claims?

VA disability claims for PTSD MST require special care and handling by the Veteran Service Representative and VA Rater assigned to your claim.
Personal trauma for the purpose of Department of Veterans Affairs (VA) disability compensation claims based on posttraumatic stress disorder (PTSD) refers broadly to stressor events involving harm perpetrated by a person who is not considered part of an enemy force.
Examples include, assault, battery, robbery, mugging, stalking, harassment.
Military Sexual Trauma (MST) is a subset of personal trauma and refers to sexual harassment, sexual assault, or rape that occurs in a military setting.
Examples of PTSD MST include the following:
- Being pressured or coerced into sexual activities, such as with threats of negative treatment if you refuse to cooperate or with promises of better treatment in exchange for sex,
- Someone having sexual contact with you without your consent, such as when you were asleep or intoxicated,
- Being physically forced to have sex,
- Being touched in a sexual way that made you uncomfortable,
- Comments about your body or sexual activities that you found threatening, and
- Unwanted sexual advances that you found threatening.
To receive disability compensation from the VA, you must have a current diagnosis of PTSD related to these experiences.
Further, there must be some evidence that the MST event occurred during military service.
Examples of direct sources of evidence include:
- Any service medical or personnel record documenting that the MST event occurred
- Department of Defense (DoD) sexual assault or harassment reporting forms
- Investigative reports completed during military service. In addition to service records or DoD reports, Veterans who have current posttraumatic stress disorder (PTSD) related to their experiences of MST can also submit alternative sources of evidence. Although these sources of evidence may not directly document the occurrence of the MST event, they may corroborate the occurrence of event.

Examples of indirect sources of evidence include, but are not limited to:
- A chaplain or clergy
- A counseling facility or health clinic
- A rape crisis center or center for domestic abuse
- A faculty member
- Civilian police reports
- Family members or roommates
- Fellow service members
- Medical reports from civilian physicians or caregivers who treated the Veteran immediately following the incident or sometime later
- Personal diaries or journals
When service records or alternative sources of evidence are not available, indirect sources of evidence may be used to establish the occurrence of an MST stressor.
These may be behavioral events, patterns of changed behavior, or circumstances that provide clues supporting a veteran’s report of the trauma.

The veteran does not have to show definitive evidence that the MST event occurred.
Some examples of PTSD MST markers include, but are not limited to:
- Change in work performance
- Anxiety
- Depression
- Panic attacks
- Pregnancy tests
- Relationship issues, like breakups, separation, or divorce
- Requests for transfer to another military duty assignment
- Sexual dysfunction
- Substance abuse
- Tests for sexually transmitted diseases
- Unexplained social or economic behavior
How Does the VA Verify a PTSD Stressor?
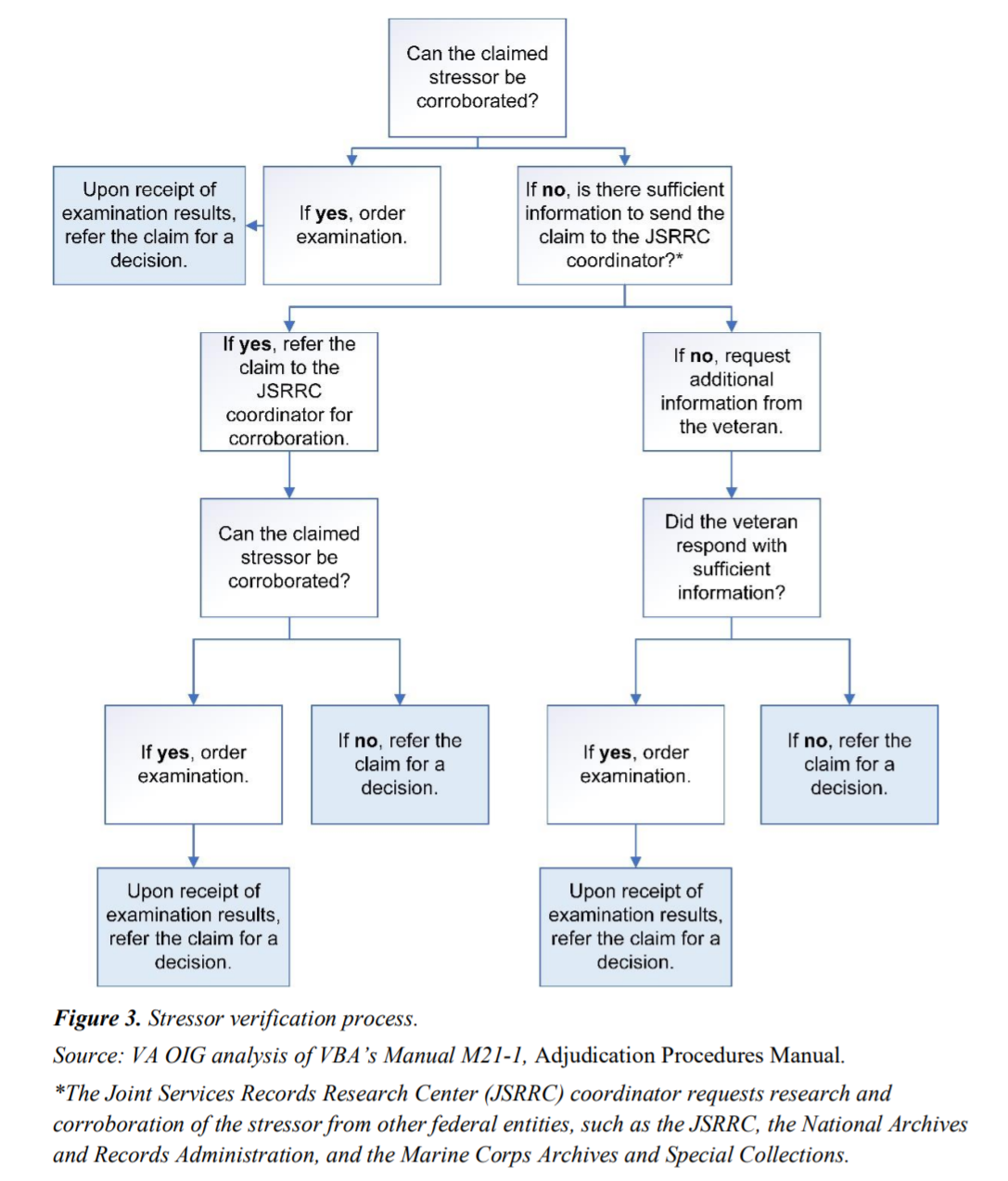
Stressor verification information can often be found in the veteran’s service records or other official documents.
When in doubt, VA Raters must verify a veteran’s PTSD stressor event through the Joint Services Records Research Center (JSRRC).
Bottom line: If the VA can’t verify your PTSD stressor event, you’ll likely have your VA claim denied.
The list below, although not all-inclusive, provides examples of the types of official service records that may be useful in stressor verification:
- Service personnel records (DD 214) and pay records
- Military occupation evidence
- Hazard pay records
- Service treatment records (STRs)
- Military performance reports
- Verification that the Veteran received Combat/Imminent Danger/Hostile Fire Pay
- Unit and organizational histories
- Daily staff journals
- Operational reports-lessons learned (ORLLs)
- After action reports (AARs)
- Radio logs, deck logs, and ship histories
- Muster rolls
- Command chronologies and war diaries
- Monthly summaries and morning reports
- Newspaper clippings and online articles
- Photographic evidence
- KIA or MIA reports
Chapter 3: Service Connection for PTSD
How Do I Get Service Connected for PTSD?
For a veteran to get service connected for disability benefits related to PTSD, the VA must have evidence of 3 evidentiary elements:
- The veteran has a diagnosis of PTSD, AND
- The stressor occurred during military service, AND
- A “Nexus” or link, established by medical evidence, between the current PTSD symptoms and the in-service stressor.
VA regulation requires that there be credible supporting evidence of a specific in-service stressor, which distinguishes claims for PTSD from other types of claims for service connection.
There are five exceptions to the requirement for credible supporting evidence that the specific in-service stressor occurred.

These exceptions are avenues that allow VA to use a reduced evidentiary standard for consideration of the in-service stressor:
- The evidence establishes a diagnosis of PTSD during service.
- The evidence establishes that the veteran engaged in combat with the enemy.
- A stressor claimed by a veteran is related to the veteran’s fear of hostile military or terrorist activity.
- Evidence establishes that the veteran was a prisoner of war.
- Evidence from sources other than the veteran’s service records corroborates the veteran’s account of a stressor based on in-service personal assault, including evidence of behavior changes following the claimed assault.
For the first four exceptions, the reduced evidentiary standard allows the veteran’s lay testimony alone (personal statement in support of a claim) to establish the occurrence of the claimed in-service stressor, if there is no clear and convincing evidence to the contrary, and the claimed stressor is consistent with the circumstances of the veteran’s service.
All other types of in-service stressors that would not fit into one of the five exceptions require credible supporting evidence that the claimed in-service stressor occurred.
Expert-Level Tips for PTSD VA Claims

Expert Tip #1: Get a medical diagnosis of PTSD before filing a claim. While the diagnosis can come from anywhere, it’s recommended that you get a diagnosis at the VA and begin treatment.
Expert Tip #2: Your PTSD stressor event must be verifiable through the JSRCC. If your stressor can’t be verified, you’ll likely be denied service connection for PTSD.
Expert Tip #3: Certain medals and citations automatically concede the stressor event, such as:
- A Veteran received one of the combat decorations cited in M21-1, Part VIII, Subpart iv, 1.A.3.h, OR
- There is other credible supporting evidence that the Veteran engaged in combat as defined in M21-1, Part VIII, Subpart iv, 1.A.3.e.
When a veteran has received any of the combat decorations listed below, VA will presume that the Veteran engaged in combat with the enemy, and concede the stressor, unless there is clear and convincing evidence to the contrary:

- Air Force Achievement Medal with “V” Device
- Air Force Combat Action Medal
- Air Force Commendation Medal with “V” Device
- Air Force Cross
- Air Medal with “V” Device
- Army Commendation Medal with “V” Device
- Bronze Star Medal with “V” Device
- “C” device, denoting combat conditions, when affixed to other awards for meritorious service or achievement
- Combat Action Badge (CAB)
- Combat Action Ribbon (CAR) (Prior to February 1969, the Navy Achievement Medal with “V” Device was awarded.)
- Combat Aircrew Insignia
- Combat Infantry/Infantryman Badge (CIB)
- Combat Medical Badge
- Distinguished Flying Cross
- Distinguished Service Cross
- Fleet Marine Force (FMF) Combat Operations Insignia
- Joint Service Commendation Medal with “V” Device
- Medal of Honor
- Navy Commendation Medal with “V” Device
- Navy Cross
- Parachutist Badge with Combat Jump Device
- Purple Heart, and/or
- Silver Star
Pro Tip: Receipt of one of the decorations cited above is not the only acceptable evidence of engagement in combat.
Note: If the Veteran does not expressly state the nature of the stressor,
- Assume the stressor is combat-related if the Veteran received one of the combat decorations cited in M21-1, Part VIII, Subpart iv, 1.A.3.h, AND
- Request service personnel records as discussed in M21-1, Part VIII, Subpart iv, 1.A.2.e.
Also note that recent military operations and warfare have involved the expansive use of armed drone aircraft, including, but not limited to, the Predator and Reaper.
Concede a stressor if the Veteran’s DD Form 214 or other service records shows service as an armed drone aircraft crew member.
What Are the Two Types of PTSD Claims?
#1. PTSD Combat Claims
PTSD combat claims include PTSD initial claims and PTSD review claims.
Initial claims for combat PTSD typically require additional development, such as stressor verification.
PTSD review claims are for veterans who are already service connected for PTSD and are seeking an increase in the rating or it’s a review of the initial PTSD rating within the first 5 years.
#2. PTSD Non-Combat Claims
There are PTSD non-combat initial claims and PTSD non-combat review claims.
This category also includes PTSD claims based on personal injury or assault, more commonly knows as PTSD MST claims.
How Do I Get Service Connection for PTSD?
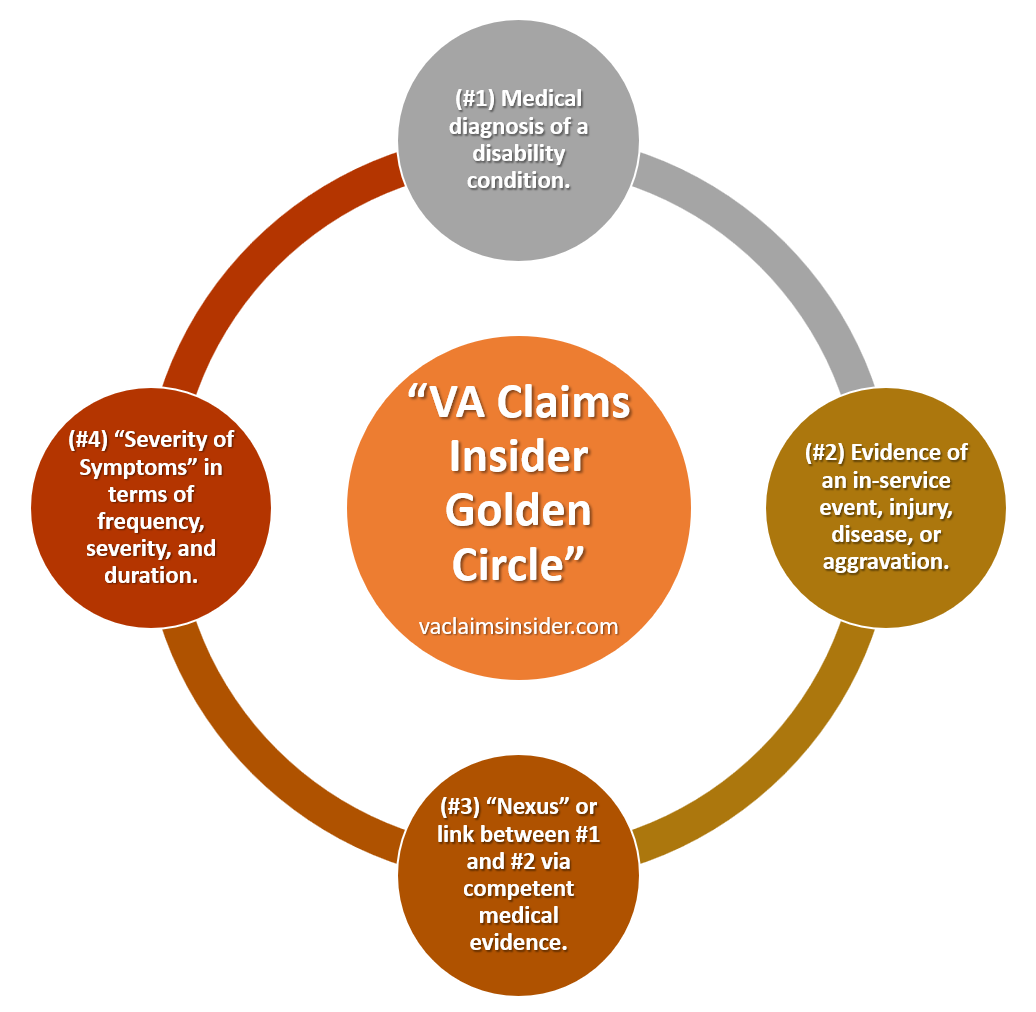
To get service connected (and rated) for PTSD, a veteran must prove 4 essential elements before the VA:
#1. Credible supporting evidence that the claimed in-service PTSD stressor event happened to you.
Every VA claim for PTSD must include a signed copy of the VA Form 21-0781, Statement in Support of Claim for Service Connection for PTSD.
Be sure to explain in-detail, along with the month and year of the events or incidents, that led to the development of PTSD.
If the PTSD claim is secondary to personal injury, sexual assault, or sexual harassment use the VA Form 21-0781a.
Veterans should also explain their current symptoms of PTSD and any impact to occupational and social impairment.
These may include explanations of the following:
- Visits to a medical or counseling clinic without a specific diagnosis or specific ailment
- Sudden requests for a change in occupational series or duty assignment
- Increased use of sick leave without an apparent reason
- Changes in job-related performance and performance evaluations
- Episodes of depression, panic attacks, or anxiety without an identifiable cause
- Increased or decreased use of prescription medications
- Increased use of over-the-counter medications
- Substance abuse such as alcohol or drugs
- Increased disregard for military or civilian authority to include rage and anger
- Obsessive behavior such as strange behaviors, overeating or under eating
- Pregnancy tests around the time of the incident
- Tests for HIV or sexually transmitted diseases
- Unexplained economic or social behavior changes to include gambling or increased spending
- Breakup of a primary relationship or difficulties in relationships
What Are Buddy Letters for PTSD?

VA Raters are required to accept a buddy letter (and concede the stressor, which means “accept” the stressor event as true) from a fellow veteran as corroboration of a claimed in-service stressor if the statement is consistent with the time, place, and circumstances of the service of both the veteran and the fellow veteran making the statement.
Thus, obtaining one or more buddy letters for stressor event verification is crucial for PTSD claims.
If you’re unable to get a Buddy Letter for PTSD, at a minimum, you should write a personal statement in support of a claim for PTSD on the VA Form 21-4138.
Be sure to list the stressor event(s), PTSD diagnosis date, the approximate date and time your symptoms began, a list of your current PTSD symptoms, and how they are negatively affecting your work, life, and social functioning.
#2. Medical evidence diagnosing PTSD in accordance with 38 CFR 4.125
Veterans must have a medical diagnosis of PTSD that conforms to DSM-V criteria to be acceptable for rating purposes by the VA.
The initial diagnosis of PTSD must come from a board-certified or board-eligible Psychiatrists, licensed doctorate-level Psychologist, or other medical providers under the close supervision of a board-certified or board-eligible psychiatrist or licensed doctorate-level psychologist.
The following credentialed mental health professionals are qualified to perform initial C&P mental disorder examinations:
- Board-certified or board-eligible psychiatrists
- Licensed doctorate-level psychologists, or
- The following other mental health professionals, under the close supervision of a board-certified or board-eligible psychiatrist or licensed doctorate-level psychologist:
- doctorate-level mental health providers
- psychiatry residents, and
- clinical or counseling psychologists completing a one-year internship or residency.
Note: “Close supervision” means that the supervising psychiatrist or psychologist met with the Veteran and conferred with the examining mental health professional in providing the diagnosis and the final assessment. The supervising psychiatrist or psychologist must co-sign the examination report.
Important: For a claim for service connection (SC) for PTSD based upon a stressor related to the Veteran’s fear of hostile military or terrorist activity, 38 CFR 3.304(f)(3) directs that the examination must be conducted by a VA psychiatrist or psychologist, or a psychiatrist or psychologist with whom VA has contracted.
The following credentialed mental health professionals are qualified to perform C&P mental disorder review examinations or examinations in claims for increased evaluations of service-connected (SC) mental disorders:
- Mental health professionals qualified to perform initial mental disorder examinations per M21-1, Part IV, Subpart i, 3.A.1.h, or
- Other mental health professionals under the close supervision of a board-certified or board-eligible psychiatrist or licensed doctorate-level psychologist, including
- licensed clinical social workers
- nurse practitioners
- clinical nurse specialists, and
- physician assistants
Pro Tip: For the VA to accept a PTSD diagnosis for rating purposes, it must conform to DSM-V Criteria.
VA PTSD Test: A Valid Diagnosis for PTSD Includes 8 Criteria (A-H)
Criterion A (one required): The person was exposed to: death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence, in the following way(s):
- Direct exposure
- Witnessing the trauma
- Learning that a relative or close friend was exposed to a trauma
- Indirect exposure to aversive details of the trauma, usually in the course of professional duties (e.g., first responders, medics)
Criterion B (one required): The traumatic event is persistently re-experienced, in the following way(s):
- Unwanted upsetting memories
- Nightmares
- Flashbacks
- Emotional distress after exposure to traumatic reminders
- Physical reactivity after exposure to traumatic reminders
Criterion C (one required): Avoidance of trauma-related stimuli after the trauma, in the following way(s):
- Trauma-related thoughts or feelings
- Trauma-related reminders
Criterion D (two required): Negative thoughts or feelings that began or worsened after the trauma, in the following way(s):
- Inability to recall key features of the trauma
- Overly negative thoughts and assumptions about oneself or the world
- Exaggerated blame of self or others for causing the trauma
- Negative affect
- Decreased interest in activities
- Feeling isolated
- Difficulty experiencing positive affect
Criterion E (two required): Trauma-related arousal and reactivity that began or worsened after the trauma, in the following way(s):
- Irritability or aggression
- Risky or destructive behavior
- Hypervigilance
- Heightened startle reaction
- Difficulty concentrating
- Difficulty sleeping
Criterion F (required): Symptoms last for more than 1 month.
- Check Yes or No
Criterion G (required): Symptoms create distress or functional impairment (e.g., social, occupational).
- Check Yes or No
Criterion H (required): Symptoms are not due to medication, substance use, or other illness.
- Check Yes or No
#3. “Nexus” or link/connection, established by medical evidence, between current symptomatology and the claimed in-service stressor.
For the VA to service connect your PTSD, you must prove a “Nexus” – meaning link or connection – between your medical diagnosis of PTSD and your stressor event.
This is accomplished at your C&P exam for PTSD by a U.S. board certified Psychiatrist or Psychologist.
The examiner will give their medical opinion as to the likelihood that your PTSD was caused or made worse by your military service.
If you’ve been out of the military for more than 12 months, the #1 best way to prove a nexus for PTSD is to get a private medical provider to write a Nexus Letter linking your PTSD to your military service and stressor.
References:
- Establishing service connection for PTSD, see
- Duty to assist with requesting records, see M21-1, Part III, Subpart i, 2.C, and
- When to request evidence from the veteran to establish an in-service stressor, see M21-1, Part VIII, Subpart iv, 1.A.2.
#4. Severity of symptoms in terms of frequency, severity, and duration, and how your symptoms negatively impact “occupational and social impairment.”
When VA Raters are determining the appropriate disability evaluation to assign for PTSD, the primary consideration is a veteran’s current SYMPTOMS based on the electronic DBQ for PTSD, however, VA Raters must also make findings as to “HOW” those symptoms impact a veteran’s “Occupational and Social Impairment.”
The #1 best way to prove your symptoms of PTSD is to have medical evidence documenting your current symptoms are how they are negatively affecting your work, life, and social functioning.
It’s also helpful to write a strong personal Statement in Support of a Claim for PTSD.
Chapter 4: VA Disability Ratings for PTSD
PTSD Basic Eligibility Criteria
To be eligible for a PTSD disability rating, a veteran must meet three (3) criteria by law:
- #1. Medical diagnosis of PTSD, in a medical record (Service Treatment Records, VA medical records, or private medical records)
- #2. Your PTSD was caused or made worse by your active-duty military service OR by another service connected disability for secondary service connection (“Nexus” for service connection)
- #3. Persistent and recurring symptoms of PTSD (“Severity of Symptoms”) to include how it affects your work, life, and social functioning
If you think you have a mental disorder such as PTSD, but don’t have a medical diagnosis, pick-up the phone and call the VA mental health facility nearest you to make an appointment right away!
If you’re trying to increase your VA rating for PTSD, you need to prove to the VA that your symptoms are now worse and warrant the higher rating criteria by law.
The #1 best way to increase your VA rating for PTSD is to have objective medical evidence to show your symptoms have worsened over time.
How Do I Get a VA Disability Rating for PTSD?
There are 3 primary ways a veteran can get a VA disability rating for PTSD:
#1: Direct service connection for PTSD rated analogous to mental disorders with a rating of 0%, 10%, 30%, 50%, 70%, or 100%.
#2: Secondary service connection for PTSD due to personal injury or assault with a rating of 0%, 10%, 30%, 50%, 70%, or 100%.
#3: Extra-scheduler rating for PTSD based on unemployability. If you’re unable to hold “substantially gainful employment” due to your PTSD, you’re eligible to receive an extra-scheduler rating based on unemployability.
How Do I Increase VA Disability PTSD?

To increase your VA disability rating for PTSD, you need to prove via medical evidence that your symptoms are worse, and warrant the higher rating criteria by law.
When VA Raters are determining the appropriate disability evaluation to assign for a mental health condition such as PTSD, the primary consideration is a veteran’s current SYMPTOMS, however, VA Raters must also make findings as to “HOW” those symptoms impact a veteran’s “Occupational and Social Impairment.”
Does the veteran’s mental health condition limit or affect his/her work, life, and/or social functioning?
The average VA rating for PTSD, across all demographics, is 70%, which is generally:
“Occupational and social impairment, with deficiencies in most areas, such as work, school, family relations, judgment, thinking, or mood.”
However, VA Raters can award a lower or higher rating (typically one level above or below) depending upon the Severity of Symptoms.
Because the use of the term “such as” in the Mental Health rating criteria demonstrates that the symptoms after that phrase are NOT intended to be an exhaustive list, VA Raters need not find the presence of all, most, or even some, of the enumerated symptoms to award a specific rating.
Nevertheless, all ratings in the general rating formula for Mental Health are also associated with observable symptomatology and the plain language of the regulation makes it clear that the veteran’s impairment must be “due to” those symptoms, a veteran may only qualify for a given disability rating by demonstrating the particular symptoms associated with that percentage, or others of similar Frequency, Severity, and Duration.
What is the Reasonable Doubt Rule for PTSD?
The reasonable doubt rule, also known as the Benefit of the Doubt Doctrine, means that the evidence provided by the claimant/beneficiary (or obtained on his/her behalf) must only persuade the decision maker that each factual matter is “at least as likely as not.”
This means there’s a 50/50 chance. When, after careful consideration of all evidence, a reasonable doubt arises regarding service origin, the degree of disability, or any other point, such doubt will be resolved in favor of the claimant.
The courts further likened the reasonable doubt rule as akin to the principle in baseball that the “tie goes to the runner.”
When in doubt, the benefit is ALWAYS given to the veteran.
Independent providers and C&P examiners must consider and give weight to the veterans self-reported symptoms when completing their mental health evaluations and DBQs.
How Does the VA Rate PTSD?
The VA rates PTSD as a mental disorder under CFR Title 38, Part 4, Schedule for Rating Disabilities, Diagnostic Code (DC) 9411, Post-Traumatic Stress Disorder.
PTSD can be rated at 0%, 10%, 30%, 50%, 70%, or 100% depending upon the Frequency, Severity, and Duration of your symptoms as well as “HOW” those symptoms affect your “Occupational and Social Impairment” – meaning your work, life, and social functioning.
What is the PTSD Compensation Chart?
The PTSD compensation chart shows the VA ratings for PTSD, ranging from 0 percent to 100 percent, with breaks at 10 percent, 30 percent, 50 percent, and 70 percent.
| PTSD Compensation Chart (2024 Edition) | VA Rating |
| Total occupational and social impairment, due to such symptoms as: gross impairment in thought processes or communication; persistent delusions or hallucinations; grossly inappropriate behavior; persistent danger of hurting self or others; intermittent inability to perform activities of daily living (including maintenance of minimal personal hygiene); disorientation to time or place; memory loss for names of close relatives, own occupation, or own name. | 100% |
| Occupational and social impairment, with deficiencies in most areas, such as work, school, family relations, judgment, thinking, or mood, due to such symptoms as: suicidal ideation; obsessional rituals which interfere with routine activities; speech intermittently illogical, obscure, or irrelevant; near-continuous panic or depression affecting the ability to function independently, appropriately and effectively; impaired impulse control (such as unprovoked irritability with periods of violence); spatial disorientation; neglect of personal appearance and hygiene; difficulty in adapting to stressful circumstances (including work or a worklike setting); inability to establish and maintain effective relationships. | 70% |
| Occupational and social impairment with reduced reliability and productivity due to such symptoms as: flattened affect; circumstantial, circumlocutory, or stereotyped speech; panic attacks more than once a week; difficulty in understanding complex commands; impairment of short- and long-term memory (e.g., retention of only highly learned material, forgetting to complete tasks); impaired judgment; impaired abstract thinking; disturbances of motivation and mood; difficulty in establishing and maintaining effective work and social relationships. | 50% |
| Occupational and social impairment with occasional decrease in work efficiency and intermittent periods of inability to perform occupational tasks (although generally functioning satisfactorily, with routine behavior, self-care, and conversation normal), due to such symptoms as: depressed mood, PTSD, suspiciousness, panic attacks (weekly or less often), chronic sleep impairment, mild memory loss (such as forgetting names, directions, recent events). | 30% |
| Occupational and social impairment due to mild or transient symptoms which decrease work efficiency and ability to perform occupational tasks only during periods of significant stress, or symptoms controlled by continuous medication. | 10% |
| A mental condition has been formally diagnosed, but symptoms are not severe enough either to interfere with occupational and social functioning or to require continuous medication. | 0% |
What is the PTSD Rating Scale?
The PTSD Rating Scale has ratings that range from 0% to 100%, with breaks at 10%, 30%, 50%, and 70%.
The average rating for PTSD is 70%.
This section will discuss the PTSD VA ratings in detail.
0 Percent Rating for PTSD
A mental condition has been formally diagnosed, but symptoms are not severe enough either to interfere with occupational and social functioning or to require continuous medication.
This means you have a formal diagnosis of PTSD, but no symptoms.
Perhaps your PTSD symptoms are controlled by continuous use of medication.
You have no occupational and social impairment at the 0% rating.
Interested in learning more about VA disability ratings for PTSD?
>> Click HERE to see the entire PTSD Rating Scale in detail
10 Percent VA Rating for PTSD
Occupational and social impairment due to mild or transient symptoms which decrease work efficiency and ability to perform occupational tasks only during periods of significant stress, or symptoms controlled by continuous medication.
Translation: You have very mild symptoms of PTSD.
Maybe you take SSRIs (antidepressants), but these medications keep your symptoms in check.
You may have minor bouts of depression and anxiety every so often, but not routinely.
30 Percent VA Disability Rating for PTSD
Occupational and social impairment with occasional decrease in work efficiency and intermittent periods of inability to perform occupational tasks (although generally functioning satisfactorily, with routine behavior, self-care, and conversation normal), due to such symptoms as: depressed mood, anxiety, suspiciousness, panic attacks (weekly or less often), chronic sleep impairment, mild memory loss (such as forgetting names, directions, recent events).
The 30 percent rating for PTSD still has mild symptoms.
Perhaps you have some depression, anxiety, suspiciousness, mild memory loss, insomnia, and panic attacks, but not very often.
Typically, you’re having panic attacks less than once per week.
While there are some PTSD symptoms at the 30 percent level, they are generally minor and there is minimal disruption to occupational and social impairment.
50 Percent PTSD VA Rating
Occupational and social impairment with reduced reliability and productivity due to such symptoms as: flattened affect; circumstantial, circumlocutory, or stereotyped speech; panic attacks more than once a week; difficulty in understanding complex commands; impairment of short- and long-term memory (e.g., retention of only highly learned material, forgetting to complete tasks); impaired judgment; impaired abstract thinking; disturbances of motivation and mood; difficulty in establishing and maintaining effective work and social relationships.
At the 50 percent VA rating for PTSD, you’re having moderate symptoms.
The biggest difference between the 30% and 50% rating is that at this level, you’re having panic attacks more than once per week and trouble in your relationships at work and in social settings.
Perhaps you don’t have any friends or just want to be alone in your house.
Maybe you’ve lost interest in activities or hobbies you once enjoyed, displaying moderate levels of depression.
You may even be divorced or can’t get along with your spouse or with your boss and coworkers anymore (angry outbursts and rage).
70 Percent VA Rating for PTSD
Occupational and social impairment, with deficiencies in most areas, such as work, school, family relations, judgment, thinking, or mood, due to such symptoms as: suicidal ideation; obsessional rituals which interfere with routine activities; speech intermittently illogical, obscure, or irrelevant; near-continuous panic or depression affecting the ability to function independently, appropriately and effectively; impaired impulse control (such as unprovoked irritability with periods of violence); spatial disorientation; neglect of personal appearance and hygiene; difficulty in adapting to stressful circumstances (including work or a work like setting); inability to establish and maintain effective relationships.
The 70 percent VA rating for PTSD has severe symptoms and is a significant jump from the 50 percent level.
70 percent is the average VA rating for veterans who are service connected and rated for PTSD.
Notice the keyword change to “deficiencies in most areas.”
Maybe you constantly check windows and doors in your home or have other obsessive rituals as you go about your day, such as a video camera monitoring system around your property.
You’re having constant panic attacks, with severe depression and anxiety.
You get lost even driving on the same roads, even with a GPS (special disorientation).
You think about suicide often, meaning you’re having thoughts or even making plans.
You are unable to establish and maintain effective relationships at work and in social settings.
You have severe anger issues and paranoia, and maybe you don’t feel comfortable leaving your own home.
100 Percent VA Disability Rating for PTSD
Total occupational and social impairment, due to such symptoms as: gross impairment in thought processes or communication; persistent delusions or hallucinations; grossly inappropriate behavior; persistent danger of hurting self or others; intermittent inability to perform activities of daily living (including maintenance of minimal personal hygiene); disorientation to time or place; memory loss for names of close relatives, own occupation, or own name.
The 100 percent rating for PTSD has the most severe symptoms under the law.
It’s rare to see a veteran exhibit the preponderance of symptoms at this level simply because they are so severe.
Notice the keyword change to “total occupational and social impairment.”
This means you have total impairment of your work and life.
Maybe you lost a job due to PTSD and are now unemployed.
Or perhaps you can’t work because your PTSD, depression, and anxiety symptoms are so severe.
This is the first time we see the introduction of delusional thoughts, hallucinations, and grossly inappropriate behavior.
Severe memory loss and occasional inability to care for oneself are now present at the 100 percent level for PTSD.
You might even require the Aid and Attendance of another person to help take care of you.
You could also be “Housebound,” meaning you spend most of your time in your home because of a permanent disability for PTSD.
What Are the Two Important Rules Affecting PTSD VA Ratings?

A big misconception among veterans is that you need to meet ALL the subjective symptoms tied with a certain rating for PTSD to get that rating.
This is NOT true!
The Rating Veteran Service Representative (RVSR) will consider all the evidence of record and will normally assign the VA rating for PTSD based upon “Preponderance of the Symptoms.”
For example, if a veteran has 3 of the symptoms from the 50 rating for PTSD and 5 of the symptoms from the 70 percent rating, the rating agency shall assign the higher rating, unless evidence of record contradicts this subjective assessment.
The opposite is also true.
For example, if a veteran has 5 of the symptoms from the 30 rating for PTSD and 3 of the symptoms from the 50 percent VA rating, the rating agency shall assign the lower rating, unless evidence of record contradicts this subjective assessment.
According to CFR 38, Part 4, Schedule for Rating Disabilities, Paragraph § 4.126, evaluation of disability from mental disorders, the RVSR (VA Rating Official) is required to consider these two rules:
Rule #1: When evaluating mental health symptoms for PTSD, the rating agency shall consider the frequency, severity, and duration of psychiatric symptoms, the length of remissions, and the veteran’s capacity for adjustment during periods of remission.
The rating agency shall assign an evaluation based on all the evidence of record that bears on occupational and social impairment rather than solely on the examiner’s assessment of the level of disability now of the examination.
Rule #2: When evaluating the level of disability for PTSD, the rating agency will consider the extent of social impairment but shall not assign an evaluation solely based on social impairment.
What Should I Expect at a C&P Exam for PTSD?

When you arrive at your C&P exam for PTSD, you’ll likely be handed a 20-question paper quiz called the PCL-5.
There are a few variations of this self-assessment measure, which may include the PCL-5, PCL-5 with LEC-5, and/or the PCL-5 with Criterion A.
The PCL-5 is a 20-item self-report measure for PTSD that assesses the 20 DSM-5 symptoms required for a PTSD diagnosis.
The PCL-5 has a variety of purposes, including:
- Monitoring symptom changes during and after treatment
- Screening individuals for PTSD
- Making a provisional PTSD diagnosis
The PCL-5 is a 20-question test of your current PTSD symptoms from the past 30 days, and each of the questions is scored between 0-4.
The C&P examiner for PTSD can make a provisional PTSD diagnosis with a minimum cutoff score of 33, and the overall PCL-5 is scored between 0-80.
For VA rating purposes, the C&P examiner is supposed to confirm at least 1 positive response in Category B and Category C, and 2 positive responses in Category D and Category E.
Be sure to read our guide: 5 Tips to Prepare for Your C&P Exam for PTSD.
Take a free VA PTSD test based on the PCL-5.
What Questions Will I Get Asked At a PTSD C&P Exam?
At a C&P exam for PTSD, the examiner wants to get to know you.
If it’s an initial exam for PTSD, you should expect to be asked a variety of question about your pre-military, military, and post-military family history, education, work, marital, legal, behavioral, and substance abuse history.
If it’s a PTSD Review (e.g., increase claim or a review within the first 5 years) exam, the examiner will only indicate any relevant history since the previous exam.
For example, here are some questions from the PTSD Initial DBQ:
- Does the veteran have a mental health diagnosis that conforms to DSM-V criteria?
- What is the veteran’s relevant social, marital, and family history?
- What is the veteran’s relevant occupational and education history?
- What is the veteran’s relevant mental health history, to include prescribed medications, and family mental health issues?
- What is the veteran’s relevant legal and behavior history?
- What is the veteran’s relevant substance abuse history?
- Are there any behavioral observations during this examination?
- Is the veteran capable of managing his/her financial affairs?
WATCH: What You Need to Know For Your PTSD C&P Exam
Chapter 5: The 31 Symptoms of a PTSD VA Disability Rating
What Are the PTSD Symptoms Reviewed by the C&P Examiner?
The C&P examiner is required to ask you about the 31 symptoms of PTSD listed on the electronic version of the PTSD DBQ form.
#1. Depressed mood
Depression (major depressive disorder) is a common and serious medical illness that negatively affects how you feel, the way you think and how you act.
Fortunately, it is also treatable.
Depression causes feelings of sadness and/or a loss of interest in activities once enjoyed.
It can lead to a variety of emotional and physical problems and can decrease a person’s ability to function at work and at home.
Depression symptoms can vary from mild to severe and can include:
- Feeling sad or having a depressed mood
- Loss of interest or pleasure in activities once enjoyed
- Changes in appetite — weight loss or gain unrelated to dieting
- Trouble sleeping or sleeping too much
- Loss of energy or increased fatigue
- Increase in purposeless physical activity (e.g., handwringing or pacing) or slowed movements and speech (actions observable by others)
- Feeling worthless or guilty
- Difficulty thinking, concentrating, or making decisions
- Thoughts of death or suicide
#2. Anxiety
Veterans with anxiety disorders frequently have intense, excessive, and persistent worry and fear about everyday situations.
Often, anxiety disorders involve repeated episodes of sudden feelings of intense anxiety and fear or terror that reach a peak within minutes (panic attacks).
These feelings of anxiety and panic interfere with daily activities, are difficult to control, are out of proportion to the actual danger and can last a long time.
You may avoid places or situations to prevent these feelings.
Symptoms may start during childhood or the teen years and continue into adulthood.
Common anxiety signs and symptoms include:
- Feeling nervous, restless or tense
- Having a sense of impending danger, panic or doom
- Having an increased heart rate
- Breathing rapidly (hyperventilation)
- Sweating
- Trembling
- Feeling weak or tired
- Trouble concentrating or thinking about anything other than the present worry
- Having trouble sleeping
- Experiencing gastrointestinal (GI) problems
- Having difficulty controlling worry
- Having the urge to avoid things that trigger anxiety
#3. Suspiciousness
Do you have trust issues with other people or have you ever been suspicious of others and their motives toward you?
Other symptoms of suspiciousness include:
- Believing that others have hidden motives or are out to harm them
- Doubting the loyalty of others
- Being hypersensitive to criticism
- Having trouble working with others
- Being quick to become angry and hostile
- Becoming detached or socially isolated
- Being argumentative and defensive
- Having trouble seeing their own problems
- Having trouble relaxing
#4. Panic attacks that occur weekly or less often
A panic attack is the abrupt onset of intense fear or discomfort that reaches a peak within minutes and includes at least four of the following symptoms:
- Palpitations, pounding heart, or accelerated heart rate
- Sweating
- Trembling or shaking
- Sensations of shortness of breath or smothering
- Feelings of choking
- Chest pain or discomfort
- Nausea or abdominal distress
- Feeling dizzy, unsteady, light-headed, or faint
- Chills or heat sensations
- Paresthesia (numbness or tingling sensations)
- Derealization (feelings of unreality) or depersonalization (being detached from oneself)
- Fear of losing control or “going crazy”
- Fear of dying
Some people experience what is referred to as limited-symptom panic attacks, which are like full-blown panic attacks but consist of fewer than four symptoms.
Although anxiety is often accompanied by physical symptoms, such as a racing heart or knots in your stomach, what differentiates a panic attack from other anxiety symptoms is the intensity and duration of the symptoms.
Panic attacks typically reach their peak level of intensity in 10 minutes or less and then begin to subside.
#5. Panic attacks more than once a week
Same as #4 above, expect you have panic attacks MORE than 1x per week.
#6. Near-continuous panic or depression affecting the ability to function independently, appropriately, and effectively
Do you live in a near constant state of fear, anxiety, panic, and depression?
The same symptoms as #4 above, just much more frequent and severe.
#7. Chronic sleep impairment
This refers to insomnia.
Do you have difficulty falling asleep or staying sleep?
Are you tired all the time?
Is your insomnia so severe that it affects/limits your work, life, and social functioning?
#8. Mild memory loss, such as forgetting names, directions, or recent events
Have youever occasionally forgotten things you should know such as names of people you’ve met, how to get certain places, or things happening in your life or in the news?
#9. Impairment of short- and long-term memory, for example, retention of only highly learned material, while forgetting to complete tasks
Highly learned material includes repetitive tasks you’ve performed your entire life.
You remember how to brush your teeth, get dressed in the morning, go to the bathroom, drive a car, count by fives, recite the alphabet, etc.
However, you’re likely very forgetful of new things.
For example, you read the paper this morning and can’t remember any of the news stories.
Your spouse tells you to clean the house and you’ll forget unless you write it down.
If you learn something new, you quickly forget how to do it and it requires practice to pick-it-up again.
Example: “I have to write down everything or I’ll forget … I keep a notepad with me at all times.”
#10. Memory loss for names of close relatives, own occupation, or own name:
This is the most severe symptoms of memory loss and are usually indicate of the most extreme mental health symptoms, often found in patients with advanced Alzheimer’s.
For example, have you ever forgotten things you should know such as names of loved ones, your job, or your own name?
#11. Flattened affect
Flattened affect refers to severe depression.
A person with “flattened affect” aka, severe depression, may not show normal emotions, facial expressions, or voice tones (monotone voice) to situations that would usually elicit an emotional response.
For example, have you ever been unresponsive to the world around you?
Have you ever had an inappropriate or no response to a positive or negative event?
Maybe your children or grandchildren recently won an award.
A normal person would smile, celebrate, and say things like “congrats!”
But when you found out, you had little to no expression, and perhaps didn’t even respond.
#12. Circumstantial, circumlocutory, or stereotyped speech
Circumstantial speech (also referred to as circumstantiality) is a communication disorder in which the focus of a conversation drifts, but often comes back to the point.
In circumstantiality, unnecessary details and irrelevant remarks cause a delay in getting to the point.
An example of circumstantial speech is that when asked about the age of a veteran’s mother at death, the speaker responds by talking at length about accidents and how too many people die in accidents, then eventually says what the mother’s age was at death.
Similarly, a veteran afflicted with this condition, for example, when asked about a certain recipe, could give minute details about going to the grocery store, the shopping experience, people there, and so on.
Circumlocutory speech is a language disorder where the patient refers to an object, event, or person, describing its characteristics instead of using its name.
“What do you cut hair with?”
A normal person would answer: “A scissors.”
Maybe you think for a while and answer with: “Well it has two circular hands on it and some sharp blades, and you put your hand in it, spread your fingers, and place it by the hair.”
Stereotyped speech refers to persistent mechanical repetition of speech or movement, sometimes occurring as a symptom of schizophrenia, autism, or other mental disorder.
Examples include rambling on-and-on, babbling, one-word answers, no answer at all, or excessive explanation of common questions and answers.
#13. Speech intermittently illogical, obscure, or irrelevant
Very severe mental health symptoms in which you have trouble holding a normal conversation, you ramble on about something completely irrelevant to the discussion or question, and often add things that don’t make sense to a normal person.
“What is your favorite color?”
A normal person would answer: “Blue” or “My favorite color is blue.”
Maybe you start with “I can’t believe how dang busy the roads were today; I’m so sick and tired of having to drive in this traffic.”
#14. Difficulty in understanding complex commands
Maybe you’re having trouble at work because your boss has asked you to create a new report, and he/she even details how you should do it.
But you don’t know how, don’t know who to ask, and can’t figure it out.
Maybe you don’t even understand what he/she has asked.
Perhaps you’re unable to follow a complex command that involves three body parts and discriminates between right and left (e.g., “Put your right thumb in your left ear, and stick out your tongue”) and you forget or can’t do it.
#15. Impaired judgment
Have you ever made bad decisions and/or didn’t think through consequences?
Examples include drunk driving, buying a $3,000 watch you can’t afford, gambling away your savings, etc.
#16. Impaired abstract thinking
Abstract thinking is a level of thinking about things that is removed from the facts of the “here and now”, and from specific examples of the things or concepts being thought about.
Abstract thinkers can reflect on events and ideas, and on attributes and relationships separate from the objects that have those attributes or share those relationships.
For example, if you have difficulty explaining concepts, events, ideas, attributes, or relationships among things, you probably have impairment of your abstract thinking.
#17. Gross impairment in thought processes or communication
Gross impairment in thought processes or communication refers to a person’s inability to effectively communicate or think clearly.
You have trouble forming a coherent thought or can’t communicate that thought clearly and effectively.
This is a very severe symptom of a mental health condition.
#18. Disturbances of motivation and mood
This is a form of depression in which you don’t enjoy doing things you used to do, or you just don’t see those activities as “fun” anymore.
Perhaps you’re constantly in a down state of depression or struggle to get out of bed in the morning.
#19. Difficulty in establishing and maintaining effective work and social relationships
Do you struggle to meet new people?
Do you find it difficult to trust other people?
Do you have very few friends at work or in your life?
Do you find yourself not wanting to go to events, meet new people, try new things, or socialize with others?
#20. Difficulty adapting to stressful circumstances, including work or a work like setting
Do you get overwhelmed easily?
Do you have to take breaks or naps when things get stressful?
Do you struggle to get started on things because your anxiety spikes?
Do you find your mind and body wandering when you know you should be trying to accomplish something?
Maybe you shut down completely, and just want to stay home, watch TV, or go to sleep.
#21. Inability to establish and maintain effective relationships
Perhaps people don’t like to be around you because of your anger issues, outbursts, difficulty communicating with others, etc.
Maybe you’ve been divorced, you can’t keep a relationship intact, and you’re not a good friend.
#22. Suicidal ideation
Suicidal ideation means wanting to take your own life or thinking about suicide.
There are two kinds of suicidal ideation: Passive and Active.
Passive suicidal ideation occurs when you wish were dead or that you could die, but you don’t have any plans to commit suicide.
Active suicidal ideation, on the other hand, is not only thinking about it but having the intent to commit suicide, including planning how to do it.
Suicidal ideation is one of the symptoms of both major depression and the depression found in bipolar disorder, but it may also occur in people with other mental illnesses, such as PTSD, or no mental illness at all.
Warning signs that you or a loved one are thinking about, or contemplating suicide include:
- Isolating yourself from your loved ones
- Feeling hopeless or trapped or stuck in severe depression
- Talking about death or suicide
- Giving away possessions
- An increase in substance use or misuse
- Increased mood swings, anger, rage, and/or irritability
- Engaging in risk-taking behavior like using drugs or having unprotected sex
- Accessing the means to kill yourself, such as medication, drugs, or a firearm
- Acting as if you’re saying goodbye to people
- Feeling extremely anxious
#23. Obsessional rituals which interfere with routine activities
Perhaps you constantly check windows, doors, and locks.
Maybe you struggle to leave your own home because you fear someone might break-in, even though you have a security system.
Other examples include:
- Walking or talking a certain way
- Performing a repetitive activity, such as locking, unlocking, and relocking a door
- Repeating precise movements like sitting up and down, blinking, or walking through a doorway a certain way
- Touching items, a specific way in a particular order or a certain number of times
- Ritualistic handwashing
#24. Impaired impulse control, such as unprovoked irritability with periods of violence
Do you suffer from anger issues, and even resort to violence?
Have you even become very angry with a co-worker or spouse, and thrown things across the room, punched a wall, or even become violent with the individual?
Can you go from 0-100 in a split second (severe anger)?
#25. Spatial disorientation
Spatial disorientation means you’re unable to determine your location or movements relative to the world around you.
Perhaps you ALWAYS must drive with a GPS, Google Maps, or Waze, even though you’re driving on roads you’ve driven hundreds of times (and still get lost).
Maybe you forget where you are, where you’re going, or why you left your house in the first place.
#26. Persistent delusions or hallucinations
Delusions are people who have it can’t tell what’s real from what is imagined.
Delusions are the main symptom of delusional disorder.
They’re unshakable beliefs in something that isn’t true or based on reality.
But that doesn’t mean they’re completely unrealistic.
Delusional disorder involves delusions that aren’t bizarre, having to do with situations that could happen in real life, like being followed, poisoned, deceived, conspired against, or loved from a distance.
These delusions usually involve mistaken perceptions or experiences.
But the situations are either not true at all or highly exaggerated.
Hallucinations are generally seeing, hearing, touching, or smelling things that aren’t really there:
There are many different types of hallucinations, including:
- Auditory hallucinations: These are when someone hears something that is not there, such as a voice or radio.
- Visual hallucinations: These cause someone to see something that is not real, such as a person or animal.
- Olfactory hallucinations: These can occur when a person smells something that is not there.
- Gustatory hallucinations: These cause someone to taste something they did not eat.
- Tactile hallucinations: These occur when a person feels like something, or someone touched them.
- Somatic hallucinations: These hallucinations can affect the entire body, causing unreal sensations such as that of bugs crawling on the skin.
#27. Grossly inappropriate behavior
Grossly inappropriate behavior is behavior that varies wildly from what a normal person would consider “appropriate” under similar circumstances.
Have you ever become extremely angry and actually threated to beat someone up?
Maybe you’ve been in bar fights.
Have you ever smashed someone’s windows because of the way they looked at you?
Perhaps your road rage led you to steer another driver off the road and you exited your vehicle and got into a verbal or physical altercation.
#28. Persistent danger of hurting self or others
Persistent danger of severely hurting self or others OR persistent inability to maintain minimum personal hygiene OR serious suicidal act with clear expectation of death.
This means you have re-occurrent periods of violence or threats of violence, whereby normal people become afraid to be around you.
Maybe you’ve attempted suicide in the past or actually hurt someone else.
#29. Neglect of personal appearance and hygiene
Physical Appearance
- Poor personal hygiene
- Not wearing suitable clothing for the weather
- Messy hair, nails, or clothes
- Unexplained weight loss
- Unusual odors (not bathing)
Nutrition
- Poor diet and nutrition
- Dehydration
Living Conditions
- Filthy home
- Not doing household maintenance
- Odd behavior and lifestyles
- Hoarding animals and/or invaluable items
- Dangerous living conditions
- Home infestations (e.g., mice, insects)
- Non-functioning utilities
- Rotten food
- Bad smells
- Threatened eviction
Health
- Not refilling medications
- Missing provider’s appointment
- Refusal to seek medical treatment for serious illness
- Decreased ability to perform routine daily activities
Behaviors
- Social isolation
- Refusing to let people that provide services into the house (e.g., utility workers, home health care providers, etc.)
- Antisocial behavior / not getting along with others
- Dangerous forgetful behavior (e.g., leaving a burning stove and going to sleep)
- Not paying the bills because they either forget or the bills are lost in the clutter
#30. Intermittent inability to perform activities of daily living, including maintenance of minimal personal hygiene
Same as #29 above, and you may even require the assistance of someone else to help take care of you, such as Aid and Attendance or Housebound.
#31. Disorientation to time or place
Disorientation refers to an altered mental state.
A person who’s disoriented may not know their location and identity, or the time and date.
It’s often accompanied with other symptoms such as:
- Confusion, or being unable to think with your normal level of clarity
- Delirium, or being confused and having disrupted attention
- Delusions, or believing things even if they’re false
- Agitation, or feelings of aggressiveness and restlessness
- Hallucinations, or seeing or hearing things that aren’t there
- Wandering around
Chapter 6: VA Disability Ratings for PTSD in 2024 – Frequently Asked Questions (FAQs)

Can I get VA disability compensation for PTSD?
Yes, the Department of Veterans Affairs (VA) will pay veterans with service-connected PTSD tax free compensation each month.
The amount of compensation depends upon your overall VA rating.
For example, a 10% rating is worth around $150 each month whereas a 100% rating is worth around $3,000 per month.
Is PTSD a VA disability condition?
Yes, PTSD is a VA disability and can be rated from 0% to 100% depending upon the severity of your symptoms.
Often, PTSD-like symptoms are actually symptoms of another mental health condition such as Major Depressive Disorder, Generalized Anxiety Disorder, Chronic Adjustment Disorder, or Somatic Symptom Disorder.
Due to the legal concept called avoidance of pyramiding, a veteran will only receive one VA rating for a mental health condition.
The VA recognizes PTSD Disorders as one of 31 mental health conditions that may be related to service, and thus, PTSD is a VA disability, and is eligible for VA compensation and benefits under the law.
What are the VA disability ratings for PTSD?
The VA will give you a disability rating based upon the severity of your PTSD, specifically related to your level of occupational and social impairment.
If you are considered service-connected for PTSD, you will receive one of six (6) possible VA disability ratings for your mental health condition, broken out as follows: 0%, 10%, 30%, 50%, 70%, or 100%.
In 2024, the average VA disability rating for PTSD is 70%.
Can I receive Special Monthly Compensation for PTSD?
Yes! VA Special Monthly Compensation under Category S is given if the veteran has at least one condition rated 100% AND one or both of the following:
#1. You are completely and permanently housebound because of his service-connected conditions, meaning that the veteran cannot leave his area of abode (this can include his own home, a hospital ward, or a care facility) at all, and this is expected to be the case for the rest of his life OR
#2. You have another condition rated 60% or group of conditions together rated 60% that are unrelated to the 100% condition. For example, you have GERD rated at 60% and Generalized PTSD Disorder rated at 100%.
Veterans can get an extra $397.88 each month, tax-free, if you meet the PTSD Disorder housebound criteria known as SMC-S.
Can PTSD be Permanent and Total (P&T)?
Some veterans may receive a permanent and total rating, also known as 100% P&T. If your PTSD Disorder is not expected to improve, you may obtain the status of permanent and total disability.
Can the VA reduce my VA disability rating for PTSD?
Yes. Unfortunately, sometimes the VA will lower a veteran’s VA rating for PTSD. If that happens to you, obtain new and relevant medical evidence for your PTSD condition, and challenge the VA’s decision to lower your rating.
How do I get a 100% VA disability for PTSD?
Your PTSD must be severe enough to warrant a 100% rating. Many veterans do obtain a higher VA rating for PTSD using VA Claims Insider’s proven proprietary education-based Coaching and Consulting process, including credible Medical Nexus Letters for Mental Health.
Can I work with a 100% VA Rating for PTSD?
Yes, you can! It is a myth that having a mental health condition somehow means you can’t work. In fact, you can work with any PTSD VA rating. Even if you’re rated at 100% for PTSD, there is no requirement or mandate that affects your work.
Will PTSD affect my security clearance?
It is a MYTH that having PTSD, or any other mental health condition will affect your security clearance. Of course, you’ll need to report it to your security manager and update your SF 86; however, it has no impact on your security clearance (in our experience serving 15,000+ veterans with a mental health condition since 2016).
Can I own a gun with a VA rating for PTSD?
Some veterans are afraid to pursue a PTSD claim, or any other mental health claim, because of concern that they will no longer be allowed to own guns.
There are prohibitions against owning a gun under certain conditions as laid forth in VA Title 18 U.S.C. § 922, such as that the applicant “has not been adjudicated as a mental defective or been committed to a mental institution,” but there is no direct prohibition against firearm ownership simply on the grounds of having a mental health diagnosis.
In real terms, that translates as being an imminent threat to yourself or others, or having been committed to a psychiatric facility by law enforcement due to threatening behavior or signs of mental illness.
Further, the VA does not automatically report veterans who apply for disability benefits based on a mental health diagnosis, and no particular PTSD or other mental health rating prohibits a veteran from purchasing or owning firearms.
The overwhelming majority of people rated for PTSD can legally own guns.
Chapter 7: Helpful VA Resources for PTSD

There are many resources available to encourage veterans to seek help or for family and friends to get educated about PTSD.
Here is a partial list:
VA’s PTSD: National Center for PTSD Police and Veteran Toolkit
National Alliance on Mental Illness (NAMI) Help Line
The NAMI Help Line is a free, nationwide peer-support service providing information, resource referrals and support to people living with a mental health condition, their family members and caregivers, mental health providers and the public.
A national telephone service of the U.S. Dept. of Veterans Affairs (VA) which aims to educate, support, and empower family members and friends who are seeking care or services for a veteran. To speak with a VA coach, call 888-823-7458, Monday through Friday, 8:00 a.m. to 8:00 p.m. ET.
- Call 1-800-273-8255 (Press 1)
- Text to 838255.
- Chat confidentially now.
An organization that provides veterans leadership and advocacy opportunities in their local communities, helping give former service members a sense of purpose and aiding them in the transition to civilian life.
Outward Bound Veteran’s Program
Outward bound provides wilderness courses and programs to build leadership and confidence among participants and offers specialized programs for veterans.
About the Author

Brian Reese
Brian Reese is a world-renowned VA disability benefits expert and the #1 bestselling author of VA Claim Secrets and You Deserve It. Motivated by his own frustration with the VA claim process, Brian founded VA Claims Insider to help disabled veterans secure their VA disability compensation faster, regardless of their past struggles with the VA. Since 2013, he has positively impacted the lives of over 10 million military, veterans, and their families.
A former active-duty Air Force officer, Brian has extensive experience leading diverse teams in challenging international environments, including a combat tour in Afghanistan in 2011 supporting Operation ENDURING FREEDOM.
Brian is a Distinguished Graduate of Management from the United States Air Force Academy and earned his MBA from Oklahoma State University’s Spears School of Business, where he was a National Honor Scholar, ranking in the top 1% of his class.